Nepal is home to eight of the world's fourteen 8,000-metre peaks. Millions of trekkers, pilgrims, and mountaineers travel here every year chasing those views, and a significant number of them walk straight into altitude sickness without ever realizing what's happening until it's already serious.
I've spent years in these mountains, accompanying guests and trekking personally on some of Nepal's most demanding high-altitude routes. And the one thing I keep seeing, season after season, is that altitude sickness doesn't discriminate!
It doesn't care how fit you are, how old you are, or how many high-altitude treks you've already completed. It is a physiological response to low oxygen, and until you're at altitude, there's genuinely no way to predict how your body will react.
So, let's break it all down. First, we'll cover what altitude sickness actually is, how it develops, and how to recognize the three types before they become dangerous.
Then, we'll move through Nepal's major trekking and climbing regions, giving you a real picture of where the risks are highest, which routes are more forgiving for beginners, and what has actually happened on these trails in recent years.
This is the guide I really wish every guest would read before departing (kudos to you that you’ve landed here!).
When you gain elevation, the atmospheric pressure drops!
At 3,000 m, you're breathing air that contains significantly fewer oxygen molecules per breath than at sea level.
And by the time you reach 5,000 m, the oxygen available per breath is roughly half of what it is at the coast. Your body doesn't adjust to this instantly, and the mismatch between what your lungs are taking in and what your tissues need is what triggers altitude sickness.
The medical term for the overall condition is hypobaric hypoxia (reduced oxygen pressure at altitude), and it affects everyone's body differently based on genetics, rate of ascent, prior acclimatization, and hydration.
The important thing to understand is that no training regimen, no fitness level, and no prior trekking experience grants immunity. Even Everest summiteers have turned back from far lower altitudes due to altitude sickness on separate occasions.
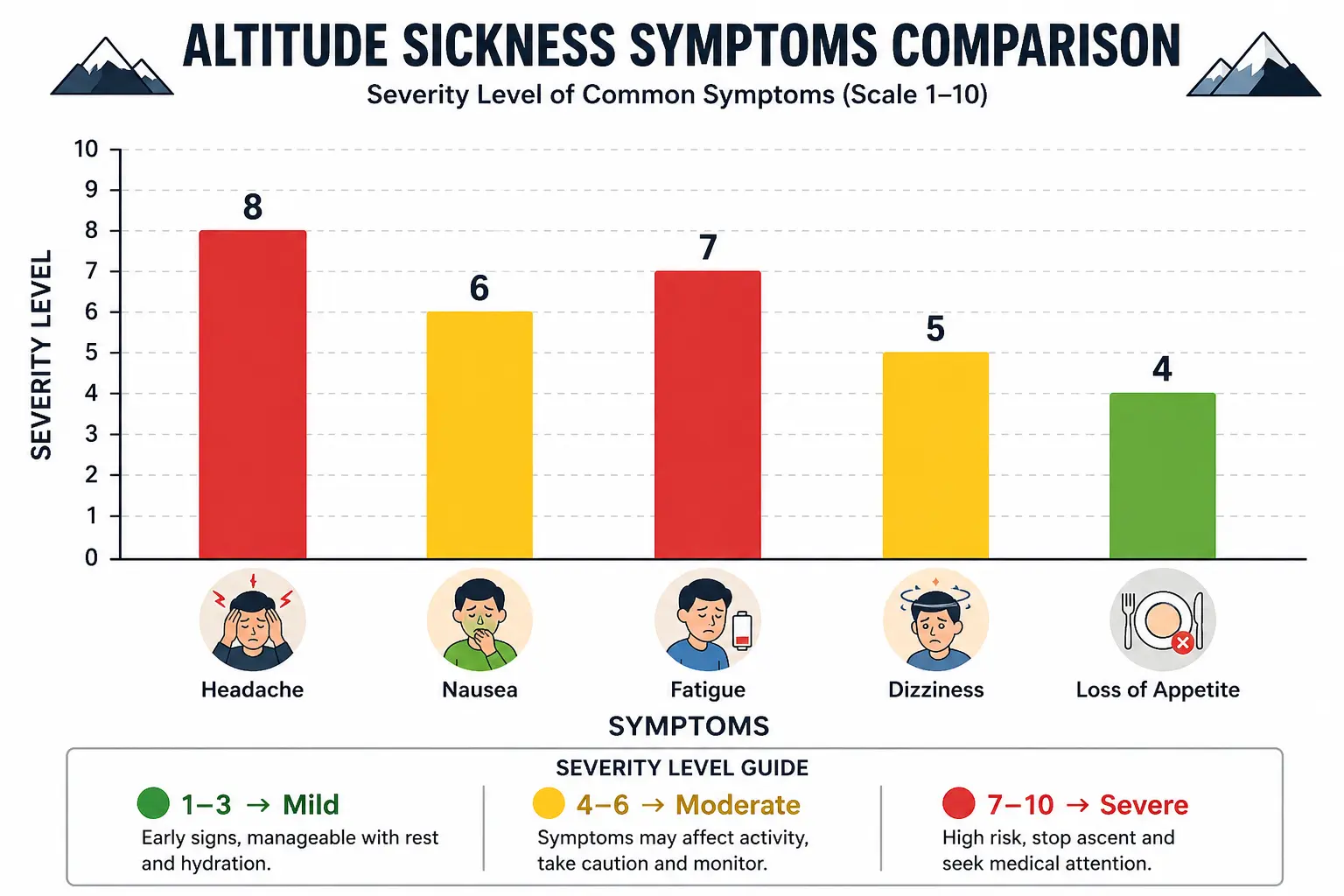
This is the part that most trekkers skim through and really shouldn't! Understanding all three forms could genuinely save your life:
AMS is the most common form, and the one you're most likely to encounter on any high-altitude trek. It typically sets in within 6 to 12 hours of reaching a higher elevation.
And the core symptoms are:
Studies show that roughly 30 to 50% of unacclimatized trekkers develop AMS symptoms above 3,500 m.
On the Everest Base Camp route specifically, approximately 40 to 50% of trekkers experience some form of AMS, with one study even claiming the figure at 40%.
The good news: mild AMS responds well to rest, hydration, and halting your ascent. The dangerous mistake is pushing through it!
HACE is severe AMS that has progressed to the point where fluid accumulates in the brain. The warning signs are very specific:
A study found that among trekkers evacuated for severe altitude illness, 21% had HACE, 27% had a combination of HACE and HAPE simultaneously (more on HAPE next).
HACE is a medical emergency, seriously! Untreated, the mortality rate approaches 50%!
However, with immediate descent, supplemental oxygen, and dexamethasone, virtually all patients make a full recovery.
HAPE is fluid accumulation in the lungs, and it is the single most common cause of altitude-related death in the Himalayas.
It usually develops 1 to 3 days after a rapid ascent and starts with following symptoms:
As it progresses,
Note that HAPE can kill within hours if the person isn't descended!
Among all the altitude emergencies our team at Adventure A One Treks has witnessed or managed over the years, HAPE is the one that always demands the fastest response.
If you see any trekker developing the symptoms above, that is not a situation to sleep on and reassess in the morning. So, kindly help your fellow trekkers in the best way possible (which is to inform the guide or taking him/her to the nearest teahouse).
Almost everyone. But here’s what you should understand on what triggered altitude sickness the most:
What does not increase your risk? Being physically unfit? Well, fitness, as multiple medical studies say, has essentially no protective effect against altitude illness!
A marathon runner and a sedentary traveller face the same baseline risk when ascending at the same rate. That's not me trying to make anyone feel better. That's simply how the physiology works!
Now let's get into the practical part of this guide, because the risk is not the same on every trail.
The Everest region is Nepal's most altitude-intensive trekking destination, and also the most medically well-equipped.
The Everest Base Camp Trek takes you from Lukla (2,860 m) all the way to Everest Base Camp at 5,364 m, with two mandatory acclimatization stops at Namche Bazaar (3,440 m) and Dingboche (4,410 m).
Most standard 12 to 14-day itineraries are well-designed for acclimatization, but trekkers who rush or skip rest days are the ones in trouble!
The Himalayan Rescue Association (HRA) operates a dedicated clinic in Pheriche (4,371 m), staffed by high-altitude medicine specialists every trekking season. Their data, compiled over decades, shows AMS incidence in the Everest region at roughly 30% among trekkers assessed at clinic level (with real community prevalence much higher).
HACE and HAPE together account for most of the serious evacuations, with the estimated altitude illness-related death rate at approximately 7.7 per 100,000 trekkers.
The Everest Three Passes Trek (Kongma La 5,535 m, Cho La 5,420 m, Renjo La 5,360 m) carries equal or higher risk simply because the altitude exposure is prolonged and the body is already fatigued when crossing each pass.
But both treks are manageable with the right itinerary. And both can be deadly if rushed.
The Annapurna Conservation Area reported 21 deaths from altitude sickness in the fiscal year 2023 to 2024, the highest of any region in Nepal!
The majority of fatalities in both years occurred around Muktinath (3,710 m), and the reason is directly connected to infrastructure. Indian pilgrims visiting the sacred Muktinath temple, Nepali day-trippers, and even some trekkers are arriving at nearly 3,800 m without a single night of acclimatization are at the prime risks!
The classic Annapurna Circuit itself (Thorong La Pass at 5,416 m, sleeping at Thorong High Camp at 4,930 m) carries significant AMS risk, with published prevalence between 34 and 57% on this route.
Studies from Manang (the main HRA aid post on the Circuit) recorded 11.6% of arriving trekkers presenting with active altitude illness.
In October 2025 alone, three porters and trekkers died near Yak Kharka (4,200 m) and Thorong La from high-altitude sickness.
Note that the Annapurna Circuit requires proper acclimatization days in Manang (3,450 m) and a rest day before Thorong La.
Annapurna Base Camp (4,130 m) is more accessible for beginners but still requires a careful pace from Chomrong (2,170 m) upward.
The Langtang region is generally the most forgiving of Nepal's major trekking destinations from an altitude sickness perspective, which is actually one of the reasons we recommend it so often for first-timers at Adventure A One Treks.
The classic Langtang Valley Trek to Kyanjin Gompa (3,890 m) stays well below 4,000 m for all overnight stays, and the gradual ascent from Syaphru Bensi (1,467 m) over multiple days gives the body excellent acclimatization time.
A published study on pilgrims attending Janai Purnima at Gosaikunda Lake (4,380 m) found AMS incidence of 34%, which tells you something important: even the Langtang region carries real risk when altitude is gained rapidly or when the destination is Gosaikunda.
Pilgrims and trekkers who ascend quickly to the sacred lake without a proper acclimatization stop below 3,500 m are the most vulnerable!
The optional hikes of Kyanjin Ri (4,700 m) and Tsergo Ri (4,985 m) in the Langtang Valley are day hikes rather than overnight stays, which means you ascend high and sleep low at Kyanjin Gompa (3,890 m), which is the exact "climb high, sleep low" principle that significantly reduces HACE and HAPE risk.
These hikes are demanding but manageable for most fit trekkers who have properly acclimatized at Kyanjin Gompa first.
The Tamang Heritage Trail (starting from Syaphru Bensi and passing through Gatlang, Thuman, and Briddhim) is the gentlest altitude profile of any major trek in the Langtang region, staying below 3,200 m throughout the Heritage section. It is genuinely the lowest-risk introductory trek for anyone concerned about altitude in Nepal.
The Manaslu Circuit is the most altitude-intensive of Nepal's major circuit treks, and remoteness is what makes it genuinely dangerous compared to the Everest and Annapurna regions.
The overnight stay at Dharmashala (4,470 m) before crossing Larke Pass (5,106 m) is the highest sleeping altitude on the circuit, and it comes after multiple consecutive long trekking days that accumulate fatigue rapidly.
The route through the Chumnubri Rural Municipality has seen increasing AMS cases, partly because new roads now allow vehicles to reach Jagat, enabling trekkers to jump-start the circuit at higher altitude than their bodies are ready for.
Local medical posts exist in Samagaun and Samdo, but helicopter evacuations are heavily weather-dependent, meaning there can be dangerous delays between when a trekker develops severe symptoms and when help arrives.
The Government of Nepal mandates a licensed guide for the Manaslu Circuit, which is both a safety requirement and genuinely good advice. Going slow, adding acclimatization days in Samagaun (3,530 m), and not skipping the Samdo (3,875 m) night before pushing to Dharmashala is non-negotiable on this route!
Beyond trekking, Nepal's high-altitude peak climbing brings altitude sickness into its most severe territory.
Island Peak (6,189 m) and Mera Peak (6,476 m) in the Everest region, Yala Peak (5,520 m) in Langtang, and Paldor Peak (5,896 m) in the Ganesh Himal range are popular trekking peaks that regularly see HACE and HAPE cases among climbers.
The summit days on these peaks involve spending hours at altitude where oxygen is less than 50% of sea level, and the physical exertion of the technical sections compounds the hypoxia significantly.
On the 8,000-metre peaks, HACE and HAPE are expected hazards at extreme altitude, and most serious expeditions carry dexamethasone, portable hyperbaric (Gamow) bags, and supplemental oxygen as standard equipment.
Even with these resources, altitude-related deaths on Himalayan expeditions occur every season!
After all of the above, here's what actually works:
Does being fit prevent altitude sickness?
No, and this is one of the most dangerous myths in Himalayan trekking. Physical fitness has essentially no protective effect against AMS, HACE, or HAPE. The body's response to low oxygen is physiological, not fitness-dependent. Elite athletes and marathon runners develop altitude sickness at the same rate as recreational trekkers when ascending at the same speed. The only things that actually protect you are: a slow ascent, proper acclimatization, and staying hydrated.
What is the lowest altitude where altitude sickness can occur in Nepal?
Symptoms can technically begin as low as 2,000 m in highly susceptible individuals, but AMS is uncommon below 2,500 m. On Nepal's trekking routes, the first real risk altitude is around 3,000 m, with the most common first symptoms appearing between Namche Bazaar (3,440 m) on the Everest trail and Ghoda Tabela (3,008 m) on the Langtang trail. Most pilgrim fatalities near Muktinath (3,710 m) and Gosaikunda (4,380 m) involve people who arrived rapidly from much lower elevations.
What is Diamox and should I take it?
Acetazolamide (brand name Diamox) is a prescription medication that accelerates acclimatization by triggering mild metabolic acidosis, which increases your breathing rate and speeds oxygen delivery to tissues. Clinical studies show it roughly halves AMS risk when taken correctly (125 to 250 mg twice daily, starting 1 to 2 days before ascent). It is not a substitute for proper acclimatization, but it is a useful safety tool for rapid ascent situations. Always consult your doctor beforehand, as it's contraindicated in sulfa allergies!
Should I carry a pulse oximeter on a trek in Nepal?
Absolutely yes, and we recommend it to every single guest we take into the field. A pulse oximeter clips to your finger and gives you a real-time reading of your blood oxygen saturation (SpO2). At Namche Bazaar (3,440 m), a healthy reading is roughly 88 to 93%. Readings below 85% at rest are a clear signal to speak to your guide and potentially descend. It's small, inexpensive, and removes a lot of the guesswork from altitude health monitoring on longer treks.
What should I do if my guide develops altitude sickness?
This is more common than most trekkers expect, especially among local Nepali guides and porters who ascend rapidly by vehicle on routes with new road access. Guides are not immune to altitude sickness just because they're local. If your guide develops symptoms, the same rules apply: halt ascent, rest, hydrate, and descend if symptoms don't improve within 24 hours or worsen at any point. Many trekking agencies, including A1 Treks, ensure that all guides carry basic altitude medications. Make sure yours does before departure.

